
A patient sits in your chair with a single missing molar, a healthy contralateral side, and a fair bit of Google research under their belt. They’ve already typed “dental bridge vs implant” into their phone and now they want your verdict: “Doctor, which one will last longer and give me less trouble over time?”
You know the honest answer is, “It depends” on biology, occlusion, habits, finances, and the quality of the lab work behind the restoration. This guide pulls together the key long term data and day to day clinical realities so you can feel confident explaining your recommendation, whether you’re planning the case yourself or partnering with a lab like NovaDent for the restorative design.
TL;DR:
- Well planned implants generally show higher 10+ year survival than tooth supported bridges in suitable patients.
- Bridges still make sense when abutment teeth already need full coverage or surgery is not an option.
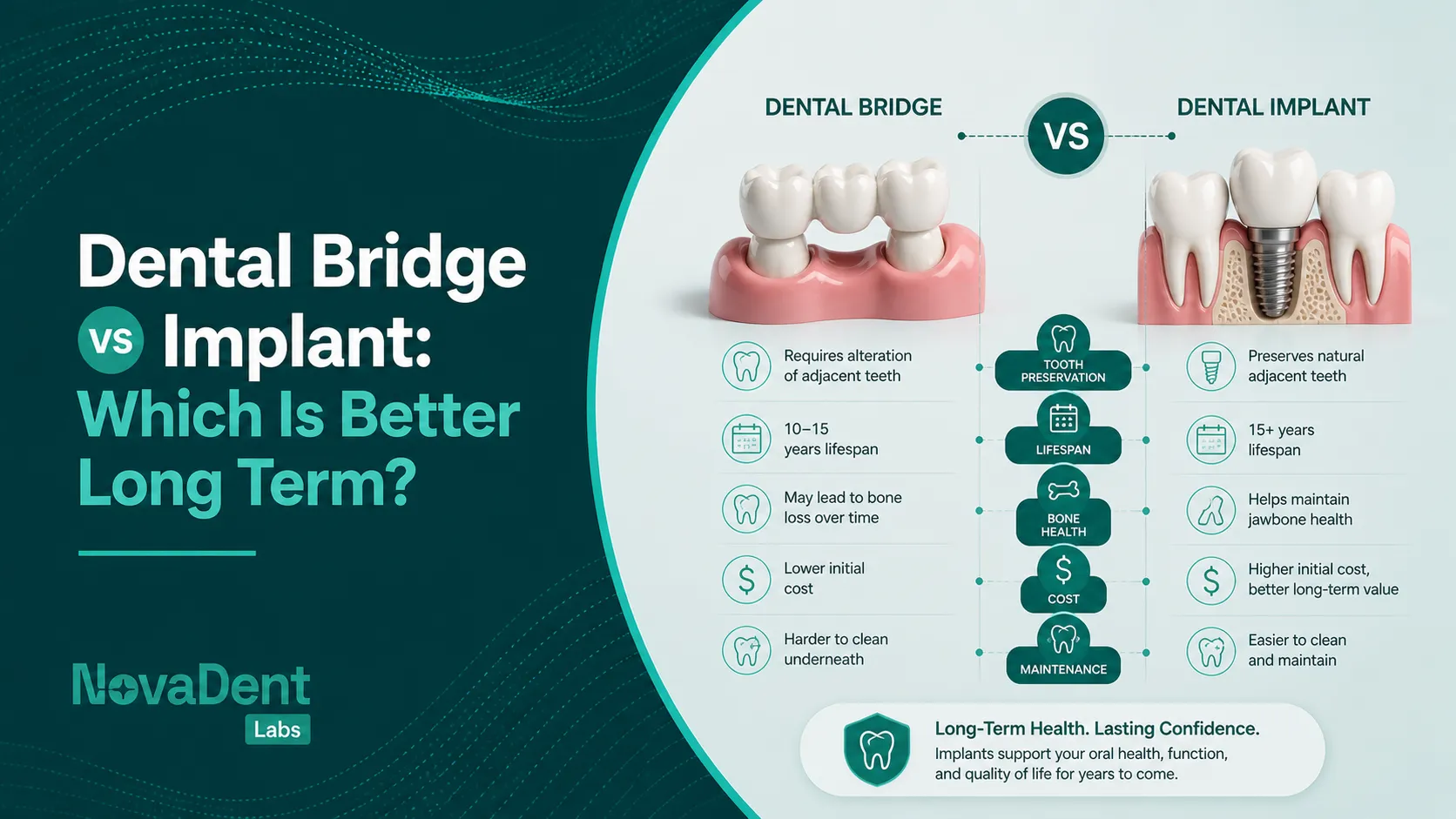
- Implants help preserve bone and spare adjacent enamel but need surgery, time and adequate volume.
- Long term success for both depends on case selection, occlusion, maintenance and lab quality.
What is the difference between a bridge and an implant?
At a glance, both options “fill the gap.” Biologically and mechanically, though, they behave very differently.

A tooth supported bridge uses neighbouring teeth as abutments, while an implant replaces the missing root directly in bone.
Tooth supported bridge
A conventional fixed dental prosthesis (FDP) relies on one or more abutment teeth. These teeth are usually prepared for crowns, and a pontic spans the edentulous space. Loads are carried through the periodontal ligament of the abutment teeth.
- Pros: No surgery, quick delivery (often within two visits), immediate improvement in function and aesthetics.
- Cons: Requires removal of sound tooth structure, higher risk of secondary caries and endodontic problems in abutment teeth over time.
For detailed material choices and design options, see our crowns and bridges service overview.
Dental implant
A dental implant replaces the root with a titanium (or zirconia) fixture placed in bone. After osseointegration, an abutment and crown or implant supported bridge are fitted on top. Loads are transmitted directly to bone without involving adjacent tooth structure.
- Pros: Preserves adjacent enamel, helps maintain bone volume, high long‑term survival in well selected cases.
- Cons: Surgical procedure, higher initial cost, longer treatment time and healing.
If your practice works digitally, you can send intraoral scans directly to NovaDent for implant planning and restorations, including custom abutments and full arch work.
Long term outcomes: how long do they really last?
Patients love the word “permanent,” but you and I know every prosthesis has a life expectancy. The question is: what does the evidence say about bridge vs implant survival over 10+ years?
Survival and complications: bridges vs implants
Systematic reviews of single tooth implants generally report 5–10 year survival in the mid 90% range, particularly for non-smokers with good oral hygiene and adequate bone. Tooth supported bridges also perform well, but multiple reviews report lower survival and more technical and biological complications over similar time frames.

Long term survival and complication rates for bridges and implants are strongly influenced by risk assessment and maintenance.
A 10 year review in the Journal of Dentistry and other journals has repeatedly shown high implant survival with controlled risk factors and good maintenance, as summarised in this 10 year implant survival data review. Bridges still have a place, but they tend to show more abutment‑related problems such as recurrent decay or the need for later endodontic treatment.
Maintenance, biology and patient behaviour
Long term success for both options hinges on plaque control, regular reviews and stable periodontium or peri‑implant tissues. For high caries risk patients who struggle with home care, a bridge supported by already heavily restored abutment teeth may be less of a gamble than placing an implant into an inflamed, poorly maintained mouth. For stable, low‑risk patients, the biological benefits of not preparing adjacent teeth often tip the scale towards implants.
When is a bridge the better choice?
There are situations where a conventional bridge still shines, especially when you already plan to crown the neighbours.
- Abutment teeth need crowns anyway. Heavily restored, cracked, or root canal treated teeth that already warrant full coverage can serve as logical abutments.
- Limited bone or anatomic constraints. Severe vertical resorption, proximity to vital structures or sinus anatomy can make implant placement risky or demand extensive grafting.
- Medical or medication related concerns. Patients with bleeding disorders, certain bisphosphonate use, or high surgical anxiety may be safer with a prosthetic solution that stays above the bone.
- Time sensitive aesthetic cases. For a fractured anterior tooth where the patient wants a fixed solution in weeks rather than months, a bridge can restore the smile quickly.
In these cases, a well designed, CAD/CAM milled bridge with sound occlusion and margins can still perform very well. NovaDent’s digital workflows for fixed prosthetics are set up to reduce chairside adjustment and support predictable outcomes over the years.
When is an implant the better choice?
For many everyday “single missing tooth” scenarios, dental implant vs bridge is less a toss up and more a question of whether the patient can proceed surgically.
- Adjacent teeth are sound. If the neighbouring teeth are untouched or have minimal restorations, most clinicians prefer to preserve enamel and use an implant supported crown instead of preparing them for a three unit bridge.
- Posterior segments with heavy function. For molar sites, an implant can carry load directly through bone and help share occlusal forces, rather than overloading two abutment teeth.
- Young and middle aged adults. These patients may need their restoration to last several decades. An implant that maintains bone and spares adjacent teeth can pay off over the long haul.
- Multi tooth gaps. Two or more implants can support a bridge and limit the number of fixtures while avoiding extended tooth supported spans.
Modern data suggest single implants can show very high survival over 10 years when risk factors such as smoking and uncontrolled periodontitis are managed. A position statement from the American Academy of Periodontology echoes this, emphasising risk based assessment and ongoing maintenance for implants used in partially edentulous patients.
At NovaDent, we routinely restore a wide range of systems and can support you with case planning, custom abutments and guided surgery stents via our digital workflow services.
Clinical decision checklist for dentists
When you are weighing bridge vs implant for a real patient rather than a textbook diagram, this structured approach helps keep things clear:
- Assess tooth prognosis. Are potential abutment teeth periodontally stable, restorable and likely to last 10+ years if crowned?
- Evaluate bone and anatomy. Use CBCT and clinical exams to gauge volume, density and distance to critical structures.
- Review systemic and behavioural risks. Smoking, uncontrolled diabetes, xerostomia and poor plaque control all change the equation.
- Consider occlusion and parafunction. Bruxism, deep overbite and group function vs canine guidance all influence design and material choice.
- Discuss cost, time and patient values. Some patients accept more visits and surgery for bone preservation; others value a simpler, shorter path.
- Involve your lab early. Share photos, radiographs and digital scans with your lab so the restoration design supports your long term plan.
Many NovaDent partner clinics send initial intraoral scans and photos even before extractions, so we can map out a staged plan for single and multi unit implant restorations.
Cost and value over the long term
Upfront, implants nearly always carry a higher fee than bridges, especially once you factor in grafting, scan based guides and custom abutments. Over 10–20 years, however, two things start to matter more than the initial quote:
- Re‑treatment and replacement. A failed bridge can mean loss of one or both abutment teeth, additional endodontics, and eventually an implant supported solution anyway.
- Tissue preservation. Maintaining bone and adjacent teeth can reduce the scale and cost of future work, particularly in younger patients.
Health economic models comparing implant supported single crowns with three unit fixed dental prostheses over 10–30 years suggest that implants can be more cost‑effective once maintenance and retreatment are included; see this implant vs bridge costs analysis as one example. Framing this as “total lifetime value” rather than simply the first bill helps patients understand why your recommendation may lean towards an implant in suitable cases.
How your lab influences long-term success
Even the best treatment plan can struggle if the lab work on the bench does not match what you saw in your chair. Marginal fit, contact strength, occlusal scheme and material selection all shape what that restoration looks like at 10 years.

Digital first CAD/CAM workflows at the lab bench help your bridge and implant cases perform predictably over the long term.
NovaDent Labs was built as a digital first lab, with CAD/CAM workflows, ISO 13485 aligned processes and TGA compliant systems. That structure is there so your bridges and implant restorations arrive with consistent fit and minimal adjustment, whether you’re working from traditional impressions or direct intraoral scans from leading systems.
If you’d like to compare fees and turnaround times for your fixed cases, you can request our price list and talk with our team about how we approach long‑term cases.
FAQs
Is a bridge or an implant better for a single missing tooth?
For a single missing tooth with healthy neighbours, most dentists now favour an implant supported crown because it preserves adjacent teeth and tends to show better long‑term survival. A bridge may still be reasonable if those neighbours already require crowns or the patient can’t proceed with surgery.
What about dental implants vs bridges for front teeth?
In the aesthetic zone, both options can work well. Implants help maintain papillae and bone, but they demand careful 3D positioning and soft‑tissue management. For thin biotypes, high smiles or compromised bones, a bridge sometimes combined with soft tissue grafting can deliver very pleasing results with less surgical risk. High‑quality lab work and communication on shade and morphology are essential either way.
Do implants really last “a lifetime”?
Studies show excellent long‑term survival for implants, but nothing is guaranteed. Peri implantitis, uncontrolled systemic disease, smoking and poor maintenance can all shorten implant life. With stable health and regular professional care, many patients can keep their implants functioning for decades.
Is a bridge easier to clean than an implant?
It depends on the design and patient. Bridges require threading under the pontic with superfloss or interdental brushes, while implants need meticulous cleaning around the collar to limit inflammation. Chairside demonstrations and written instructions built into your handover are just as important as which option you choose.
Related Posts
You may also be interested in

TMJ Splint vs Night Guard: What’s the Difference?

How to Clean a Mouth Guard Properly Without Damaging It

Multi Unit Abutment Explained: Purpose, Benefits & Applications

NovaDent Has Arrived.
Previously VTS Dental Labs.
Same team
Same standards
New identity
Visit our new website