
TL;DR
- Severe maxillary atrophy doesn’t always mean extensive grafting; zygoma based solutions can restore function with immediate full arch loading in the right hands.
- Careful case selection, sinus and soft tissue management, and a predictable prosthetic plan are essential to keeping complications in check.
- A lab experienced in full arch and zygoma cases can stabilize the workflow: digital planning, screw access, framework design and occlusion all matter.
- Talking about zygomatic implants cost is easier when you understand the surgical and lab drivers behind the fee.
Every clinician has had that CBCT moment: a maxilla so resorbed that conventional full arch implants feel like wishful thinking. The patient is motivated, medically stable and asking for fixed teeth, yet extensive multi stage grafting just doesn’t fit their life. In those situations, zygomatic implants can move the case from “nearly impossible” to “carefully doable” when placed by an experienced surgeon with a clear restorative plan.
This article is written for clinicians who already manage full-arch cases and want a structured way to think about indications, All on 4 hybrids, risks, and the lab choices that keep advanced work predictable. We’ll stay at the level of clinical decision making and prosthetic planning rather than teaching you how to operate.
This content is for dental professionals only and does not replace your own clinical judgement, local guidelines, or formal training.
What are zygomatic implants in full-arch dentistry?
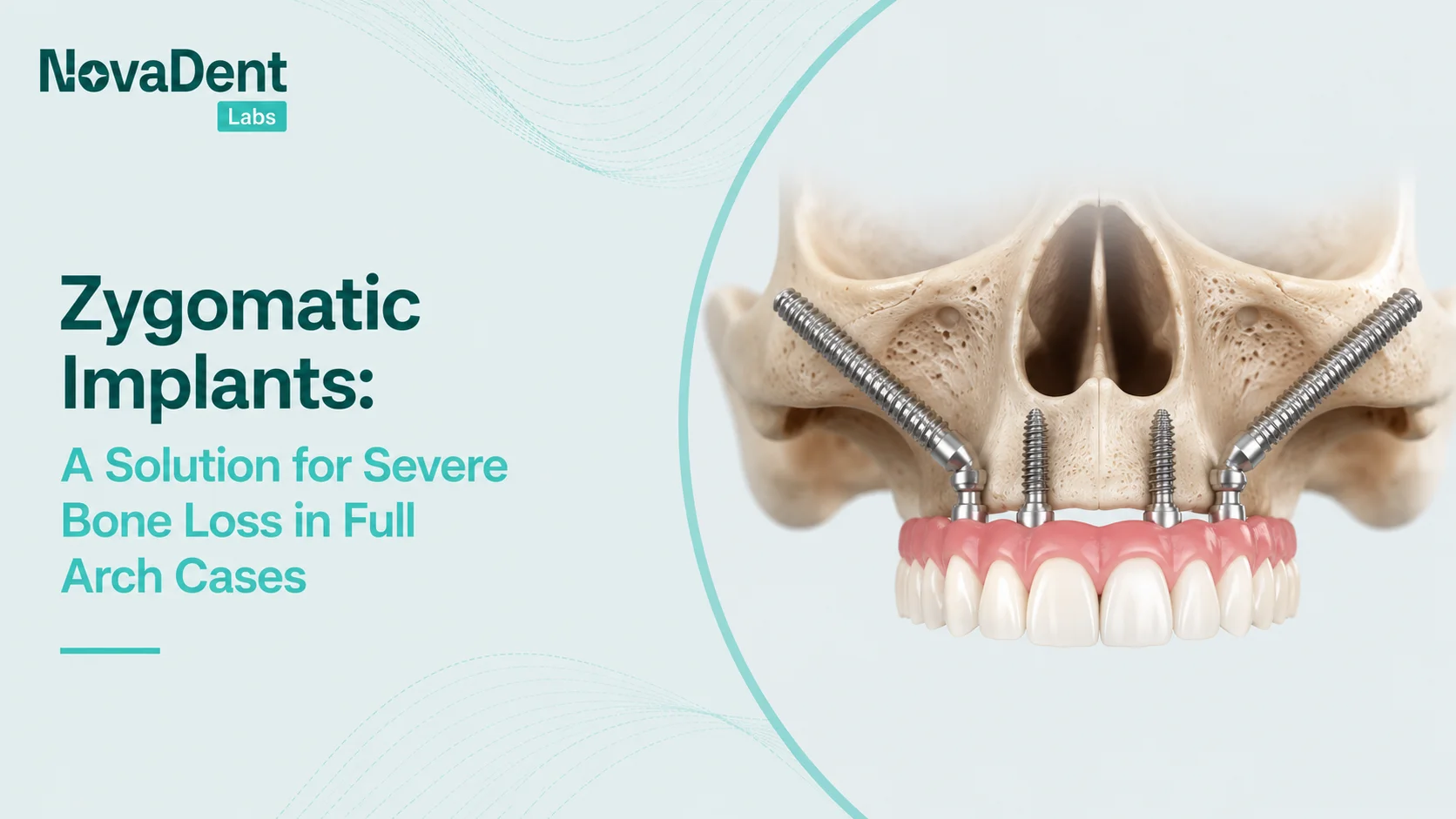
Zygomatic dental implants are extra long fixtures anchored in the body of the zygoma rather than the residual maxillary alveolus. Lengths typically range from around 30 mm up to 50 mm, allowing engagement of dense zygomatic bone even when the posterior maxilla is heavily resorbed or pneumatized.

Visualising how long zygomatic implants engage dense zygoma bone in a severely resorbed maxilla.
Instead of sinus grafts and large onlay blocks, the zygoma itself becomes the primary anchorage point. In full arch cases this can mean:
- One zygomatic fixture per side combined with anterior conventional implants, or
- A “quad zygoma” arrangement with two fixtures per side when the anterior bone is also lacking.
Modern systems pair these fixtures with angulated multi unit abutments and immediate load protocols, so a fixed provisional can often be delivered on the day of surgery using a digital or conventional workflow.
If you’re already comfortable with full arch work, that basic biology biomechanics picture will feel familiar; what changes is the anatomy you rely on, and the margin for error.
When should you consider zygomatic dental implants?
Systematic reviews and consensus statements are fairly consistent on the core indications. In brief, zygoma based solutions are most often used when you have severe maxillary atrophy or deficiency that makes conventional fixtures and standard grafting less predictable, more morbid, or both.
Typical scenarios include:
- Extremely resorbed posterior maxilla with maxillary sinus pneumatization and limited subnasal bone.
- Failed sinus grafts or onlay grafts where further grafting feels like a poor bet for the patient.
- Patients with medical or psychosocial factors that make multi stage grafting undesirable.
- Post oncologic or trauma cases where large segments of the maxilla have been lost.
Across these indications, published series and meta-analyses report high implant survival in the short to medium term, often in the mid‑90 % range, with prosthetic survival similarly encouraging. Complications such as sinus pathology, oro‑antral communications, and soft tissue issues do occur, which is why good patient selection, surgical experience, and restorative planning are non‑negotiables.
For many referrers, the practical question is not “Can zygoma work?” but “When is this the simpler overall journey for my patient than years of grafts?” That is where a structured comparison with other full arch strategies helps.
All on 4 vs all on 4 zygomatic implants vs grafting
The All on 4 concept has reshaped how we think about graftless full arch rehabilitation: four fixtures (two anterior axial, two posterior tilted) supporting an immediate fixed bridge. Systematic review of long term outcomes with All on 4 full arch prostheses. In moderately atrophic maxillae, that alone can be enough.
When posterior and sometimes anterior bone are severely compromised, surgeons may add one or more zygoma fixtures to create an All on 4 zygomatic hybrid or even a quad zygoma configuration, still aiming for same day fixed loading.
The “right” choice turns on more than bone volume: patient expectations, comorbidities, travel distance, and financial realities all matter. A good starting point is to map both a graft based path and a zygoma based path and discuss them with the patient in everyday language.
For a refresher on conventional full arch options, you may find it helpful to review your lab’s implant restorations overview alongside this article.
Clinical workflow: from CBCT to immediate load
In zygoma supported full arches, the surgery and the prosthesis are tightly linked: a technically beautiful quad zygoma with unreachable screw channels or an unwearable occlusion is still a failure in the patient’s eyes. Most teams find the following workflow components helpful:

Joint digital planning between surgeon, restorative dentist and lab helps de‑risk zygomatic full arch workflows.
1. Preoperative records and planning
- High quality CBCT with clear visualisation of the zygoma, sinus and residual crest.
- Intraoral scans or well made impressions and jaw relation records.
- Photos or video of smile line, lip dynamics and profile to plan vertical dimension and tooth display.
- Discussion with your lab around ideal screw access, anterior posterior spread, and available restorative space.
NovaDent integrates your planning software and guide provider with our digital workflows so planned implant positions remain compatible with a prosthesis you can actually deliver on day one.
2. Day of surgery prosthesis
- Pre-made, tooth positioned PMMA or printed prosthesis based on a wax up or virtual setup.
- Intraoperative verification jig or similar strategy to confirm framework passivity.
- Careful adjustment of occlusion in centric with shallow anterior guidance to keep forces in check.
3. Transition to the definitive prosthesis
- Healing period with regular review for soft tissue health and sinus related symptoms.
- Conversion of the provisional into a digital blueprint: scan bodies, bite records, photos.
- Decision on material stack (e.g., milled titanium + composite, full contour zirconia with careful design, or hybrid options) based on parafunction, esthetics and budget.
Case vignette: immediate load zygoma solution
A 67 year old patient from regional NSW presented with a failing upper denture, advanced posterior maxillary resorption and a strong preference to avoid multiple grafting surgeries. CBCT showed minimal posterior bone height and limited premaxillary support, so the team planned two anterior conventional fixtures plus bilateral zygomatic implants to support an immediate load full arch. A tooth-positioned provisional was designed in advance, with screw access mapped digitally to stay within the occlusal table.
On surgery day, the patient left with a fixed provisional and acceptable phonetics; at conversion, that prototype was scanned and used as the template for a milled titanium framework with layered composite. Key learning: investing in joint planning around screw access and restorative space can save multiple review appointments and prevent compromises on occlusion.
A short shared checklist between surgeon, restorative dentist and lab before surgery can eliminate many headaches later. For a wider view of how this sequencing fits into complex reconstruction, you can pair this article with our full mouth rehabilitation guide and the digital dentistry workflows article.
Key lab considerations in zygoma supported full arches
From the lab side, zygomatic and hybrid All on 4 cases succeed or struggle on a handful of recurring details:
- Screw channel emergence: Zygoma trajectories can land you in the palate, buccal corridor, or incisal edges if planning is off. Joint review of the digital plan helps keep access in restoratively acceptable zones.
- Framework design and passivity: Long span, multi implant frameworks on zygoma fixtures demand meticulous virtual design, verification jigs, and high quality milling or laser sintering.
- Soft tissue support: Proper contouring to avoid food traps and allow hygiene, while respecting what the surgical soft tissue can realistically tolerate.
- Occlusion and parafunction: Many zygoma candidates have long standing functional shifts; designing shallow guidance and broad contacts can mitigate risk of overload.
As a clinician led lab, NovaDent treats complex full arch implant cases, including situations where zygomatic implants are being placed by your surgeon, as co-managed work. Our team can join planning discussions, review CBCT based designs and suggest framework strategies that match your preferred implant system and practice philosophy.
Talking about zygomatic implants cost with patients
Many clinicians wonder how to explain zygomatic implant fees when patients already find full arch numbers confronting.

Positioning zygomatic implants cost within the overall treatment journey can make fee discussions more comfortable.
While exact zygomatic implants cost structures vary by country and provider, the major drivers are consistent:
- Additional surgical time and expertise, often in a hospital or advanced sedation setting.
- More complex hardware: extra long fixtures, dedicated multi unit abutments, and sometimes custom components. Nobel Biocare data on NobelZygoma implant components.
- Prosthetic complexity: extended frameworks, higher design time, more follow up visits.
- Risk management: contingency planning for sinus issues or other complications.
In Australia, published consumer guides for full arch implant treatment commonly quote around AUD $20,000–$40,000 per arch for standard All on 4 style cases, with upper arch rehabs involving zygomatic implants often sitting toward the upper end of that band or higher (for example AUD $30,000–$45,000+ depending on materials, setting and whether hospital fees are included). These are broad ranges only; each surgeon and clinic will structure fees differently, so it is safest to frame any figures you mention as indicative and defer to your surgeon partner’s written quote.
Patients generally respond well when you frame fees around the total journey: fewer surgeries, a faster path to fixed function, and a single integrated plan rather than “one more graft and we’ll see.” From the lab side, we’re happy to provide clear, written quotes so your team can give confident estimates without talking in the dark.
For a high level overview of our turnaround times, and to request a current price list, you can refer to our turnaround times and price list page.
Chairside checklist: is this a zygoma, All on 4, or graft case?
Here’s a pragmatic, non-exhaustive checklist you can run through when staring at that challenging CBCT. A quick way to structure it is to use the BONES chairside checklist Bone, Old grafts, Needs, Expertise, Support.
As you apply BONES to the scan and history, run through practical questions such as:
- Is posterior bone height and density adequate for tilted fixtures without entering the sinus unfavourably?
- Is there enough anterior bone for at least two conventional fixtures with acceptable A–P spread?
- Has the patient already undergone failed grafting, or do they strongly prefer to avoid more grafts?
- Do you have a trusted surgeon with formal training and experience in zygoma placement?
- Have you and your lab mapped likely screw access points and restorative space?
- Can the patient commit to the review schedule needed to monitor sinus and soft tissue health?
When several answers point towards zygoma, a joint planning session between surgeon, restorative clinician and lab is often the most valuable “appointment” in the whole case.
How NovaDent Labs supports advanced full-arch cases
NovaDent Labs supports referring teams with complex full arch maxillary cases, including severe atrophy, immediate load All on 4 style restorations and other advanced implant restorations, by keeping the restorative side as calm and predictable as possible.
Typical support for complex full arch implant cases includes:
- Review of CBCT derived plans from your planning software and feedback on restorative feasibility.
- Design and fabrication of immediate load provisionals (printed or milled) based on a shared aesthetic setup.
- CAD/CAM frameworks with verification steps built into the workflow.
- Clear lab sheets and case notes to keep everyone on the same page.
If you’d like a second set of eyes on an upcoming case, you can reach out via our contact page or include us early when you’re planning your next series of full arch consults.
FAQs
Which patients are good candidates for zygomatic dental implants?
Broadly, patients with severe posterior maxillary atrophy, failed previous grafting, or conditions that make grafting less desirable may be candidates, provided their general health, sinus anatomy and expectations align with the higher demands of this approach. Case selection should always be done by a clinician with specific training in zygoma surgery.
How do you explain zygomatic implants' cost to patients?
Many clinicians find it helpful to compare the full journey: multiple grafts and delayed loading over years versus a single, higher complexity procedure that aims for immediate fixed function. Breaking the fee down into surgical, prosthetic and review components gives patients a sense of what they’re investing in, rather than just a single large number.
When should you think about all on 4 zygomatic implants instead of grafting?
Consider all on 4 zygomatic implants when conventional All on 4 cannot achieve stable support in the posterior maxilla, when the patient strongly wishes to avoid grafting, or when prior grafts have already failed. In borderline cases, presenting both paths and documenting the discussion is usually the safest approach.
Related Posts
You may also be interested in

TMJ Splint vs Night Guard: What’s the Difference?

How to Clean a Mouth Guard Properly Without Damaging It

Multi Unit Abutment Explained: Purpose, Benefits & Applications

NovaDent Has Arrived.
Previously VTS Dental Labs.
Same team
Same standards
New identity
Visit our new website